The Babinski sign, also called the extensor plantar reflex, is one of the most recognized and clinically important neurological signs. It serves as a vital bedside tool to detect upper motor neuron (UMN) lesions, especially those involving the corticospinal (pyramidal) tract. Named after the French neurologist Joseph Babinski, this sign has remained a staple in neurological examinations for over a century.
1. Historical Background and Biography
Joseph Jules François Félix Babinski (1857–1932) was a prominent French neurologist of Polish descent. A student of the famed Jean-Martin Charcot, Babinski became one of the leading figures in late 19th and early 20th-century neurology.
In 1896, at a meeting of the Société de Biologie in Paris, Babinski presented a new clinical observation: stroking the sole of the foot could induce upward movement of the big toe (dorsiflexion) in patients with neurological disease — a response that contrasted with the typical downward movement (plantar flexion) seen in healthy individuals. This finding, later named the Babinski sign, became a critical clinical tool for distinguishing organic neurological disease from functional or hysterical disorders.
2. Description of the Babinski Sign
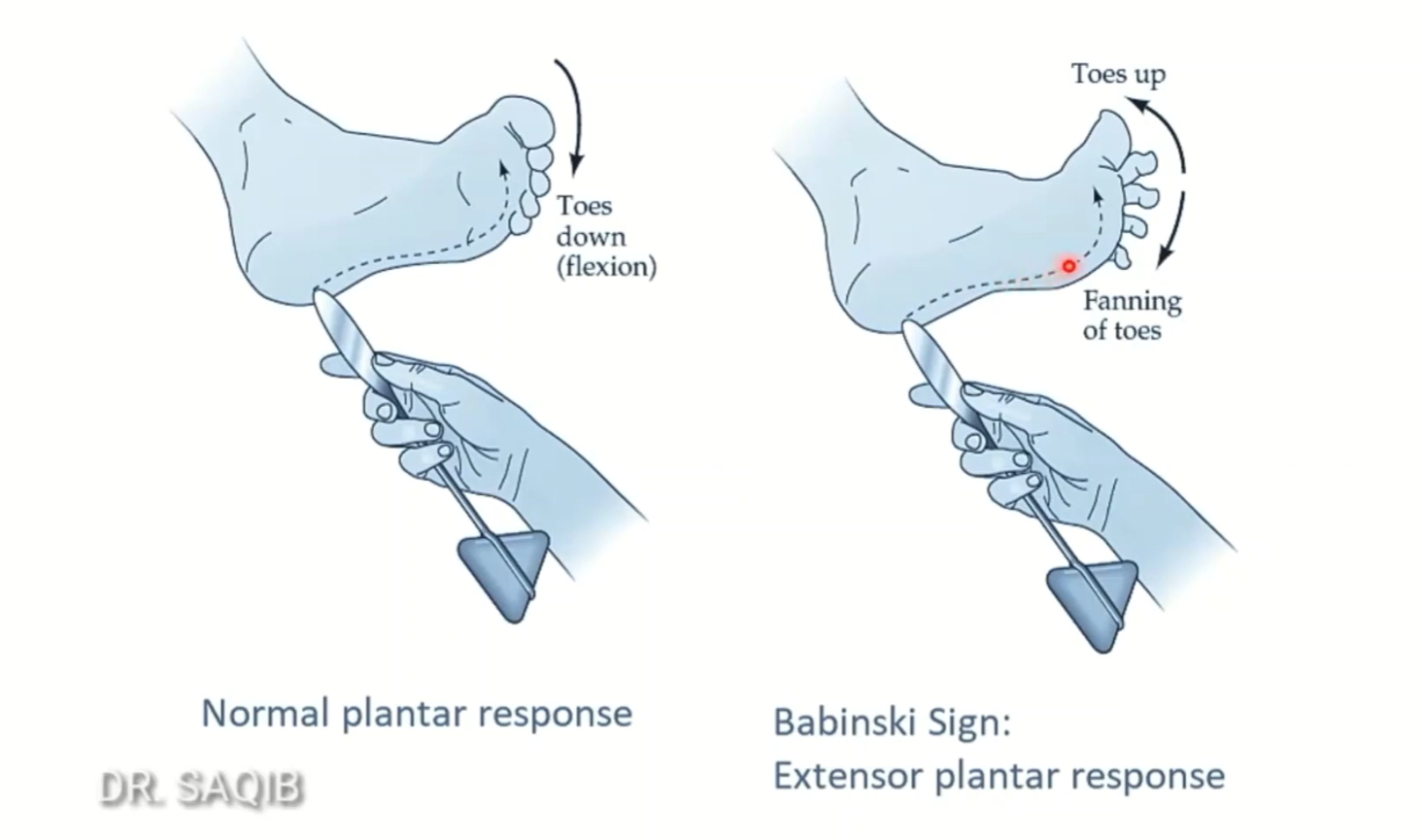
How It Is Elicited:
The examiner strokes the lateral aspect of the sole, from the heel along the outer edge toward the base of the toes, using a blunt instrument.
A positive Babinski response is dorsiflexion of the big toe, often with fanning of the other toes.
Normal vs. Abnormal:
In normal adults, the response is flexion of all toes.
In individuals with UMN lesions, the abnormal extensor response occurs.
This sign is normal in infants up to approximately 12–24 months, due to incomplete myelination of the pyramidal tracts.
3. Clinical Significance
A positive Babinski sign suggests a lesion of the corticospinal tract and is commonly seen in:
Stroke
Multiple sclerosis
Spinal cord injury
Amyotrophic lateral sclerosis (ALS)
Traumatic brain injury
The Babinski sign remains essential in neurological localization, especially in resource-limited environments or before imaging is available.
4. Differential Use and Related Signs
When the Babinski sign is equivocal, other reflexes — known as Babinski-like signs — can be used to corroborate findings. These include:
Chaddock sign – stroking around the lateral malleolus
Oppenheim sign – stroking down the medial tibia
Gordon sign – squeezing the calf muscle
All aim to provoke the same extensor plantar response and help diagnose UMN dysfunction.
5. Babinski’s Broader Contributions
Beyond the Babinski sign, Joseph Babinski made several other lasting contributions to neurology:
Pithiatism: He coined this term to distinguish hysterical disorders that respond to suggestion from true organic disease, reinforcing the importance of careful neurological differentiation.
Anosognosia: In 1914, he introduced this concept to describe patients unaware of their deficits, such as hemiplegia — a foundational idea in neuropsychology.
Neurosurgical Foundations: Babinski laid the groundwork for modern neurosurgery in France, mentoring pioneers such as Clovis Vincent and Thierry de Martel.
6. Legacy and Eponymous Syndromes
Several medical syndromes bear Babinski’s name, including:
Anton–Babinski syndrome: Cortical blindness with denial of blindness
Babinski–Nageotte syndrome: A medullary brainstem syndrome
Babinski–Fröhlich syndrome: Also known as adiposogenital dystrophy
His sharp observational skills and emphasis on objective clinical signs solidified his place in neurology’s pantheon.
7. Summary Table: Babinski Sign Overview
8. Conclusion
The Babinski sign is not only a reflex — it is a clinical legacy. It represents the power of bedside observation in an era long before imaging, and continues to teach generations of physicians how to distinguish functional from organic disease, peripheral from central injury. Joseph Babinski’s name lives on in every toe stroke that helps reveal hidden pathology — a lasting tribute to the art and science of neurology.
Comment