Bell’s Palsy: Sudden Facial Paralysis of Peripheral Nerve Origin
Bell’s palsy is a condition marked by acute, unilateral facial weakness due to peripheral facial nerve (cranial nerve VII) dysfunction. It is the most common cause of sudden facial paralysis and is typically idiopathic, though viral inflammation is suspected.
1. Historical Background and Eponym
Sir Charles Bell (1774–1842) was a Scottish neurologist and anatomist. He conducted pioneering work in neuroanatomy and demonstrated the separate motor and sensory functions of spinal nerve roots. He first described the syndrome of unilateral facial paralysis linked to facial nerve dysfunction, which later became known as Bell’s palsy.
2. Clinical Features
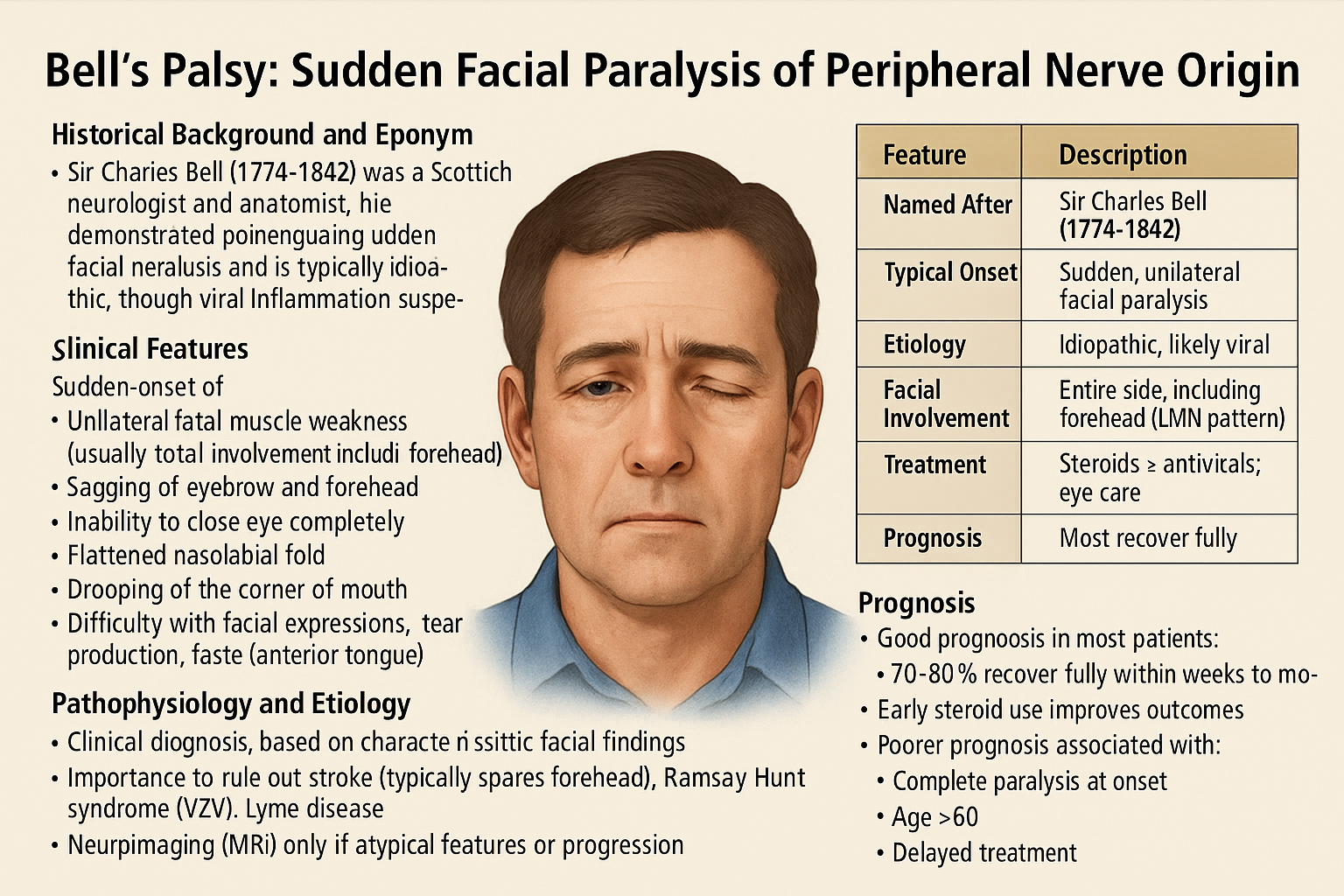
Sudden-onset of:
Unilateral facial muscle weakness (usually total involvement including forehead)
Sagging of eyebrow and forehead
Inability to close the eye completely
Flattened nasolabial fold
Drooping of the corner of the mouth
Difficulty with facial expressions, tear production, taste (anterior tongue)
3. Pathophysiology and Etiology
Likely due to viral-induced inflammation (e.g., herpes simplex virus) causing swelling of the facial nerve within the facial canal (fallopian canal)
The swelling impairs neural conduction, resulting in lower motor neuron dysfunction
4. Diagnosis
Clinical diagnosis: based on characteristic facial findings
Important to rule out: stroke (which typically spares the forehead), Ramsay Hunt syndrome (VZV), Lyme disease
Neuroimaging (MRI) only if atypical features or progression
5. Management
Corticosteroids (e.g., prednisone) – most effective if started within 72 hours
Antivirals (e.g., acyclovir) – sometimes added if viral cause suspected
Eye protection: artificial tears, patching, lubrication for incomplete closure
Physical therapy: for facial muscle stimulation and prevention of synkinesis
6. Prognosis
Good prognosis in most patients:
~70–90% recover fully within weeks to months
Early steroid use improves outcomes
Poorer prognosis associated with:
Complete paralysis at onset
Age >60
Delayed treatment
Comment