Bornholm Disease: A Viral “Devil’s Grip” of Chest Pain
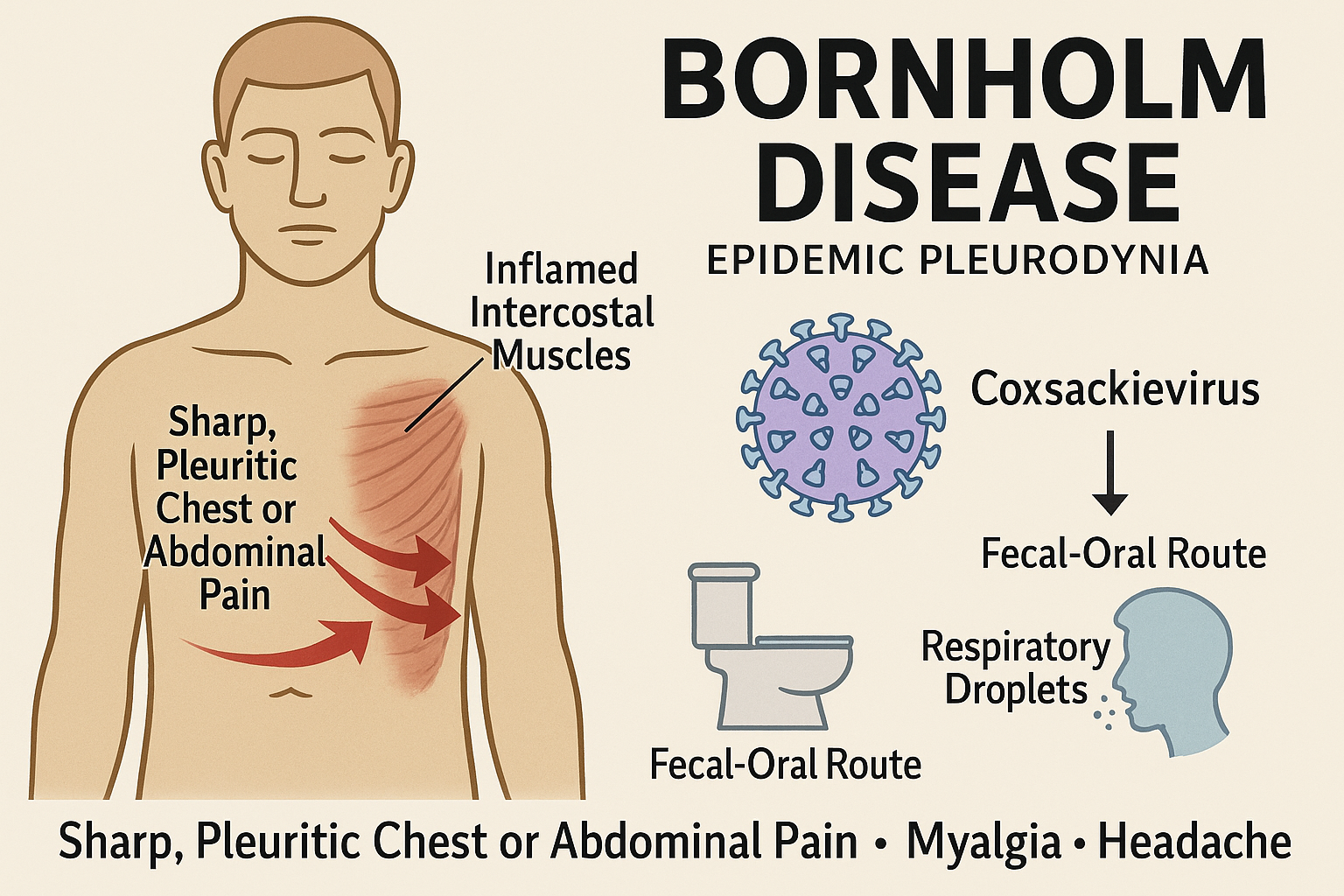
Bornholm disease is an acute, self-limited infection characterized by sudden onset of sharp chest or upper abdominal pain, often described like a “gripping” or “clutching” pain. It is most commonly caused by the Coxsackie B virus and is also known as epidemic pleurodynia.
The disease is notable for its dramatic presentation yet generally benign course.
1. Historical Background and Eponym
The condition takes its name from Bornholm Island in Denmark, where a major outbreak occurred in 1930 and caught the attention of clinicians. The term “devil’s grip” (Latin: la poigne du diable) has been historically used to describe the intense chest or abdominal pain.
2. Etiology, Transmission & Pathophysiology
Causative agents: Primarily Coxsackie B viruses (serotypes B1-B6); occasionally Coxsackie A viruses or echoviruses.
Transmission: Fecal-oral route, respiratory droplets, and direct contact with infected secretions.
Pathophysiology: The virus infects skeletal muscle, especially intercostal and diaphragmatic muscles, causing myositis. It may also involve the pleura (leading to pleuritic pain) or rarely the pericardium. Inflammation and muscle spasm result in sharp episodic pain, typically worsened by breathing or movement.
Incubation period: Approximately 2-5 days. The illness often occurs in epidemics in summer or early autumn, especially among children and adolescents.
3. Clinical Presentation
Onset: Sudden fever, chills, malaise, headache.
Pain: Sharp, stabbing or squeezing chest pain (or upper abdominal) that can mimic pleurisy or myocardial infarction. Usually unilateral, but may shift side or become bilateral; worsens with deep breathing, coughing or movement.
Tenderness: Intercostal muscle tenderness and mild pleural friction signs.
Other features: Sore throat, cough, myalgia, sometimes nausea or vomiting — especially in younger children.
Duration: Typically 2–7 days; may have relapses or prolonged pain up to 2 weeks.
Associated complications (rare): Myocarditis, pericarditis, orchitis/epididymitis (in males), aseptic meningitis.
4. Diagnosis
Clinical suspicion: Sudden chest pain during an epidemic setting, especially with muscle tenderness and viral prodrome, and normal imaging for pulmonary causes.
Investigations:
Chest X-ray: usually normal (helps exclude pneumonia or pleural effusion).
Laboratory: mild leukocytosis, slightly elevated C-reactive protein or ESR.
Viral serology or PCR: can identify Coxsackie infection but usually not required for routine care.
Key exclusion: Rule out serious conditions such as pulmonary embolism, acute coronary syndrome, pericarditis or pneumonia.
5. Differential Diagnosis
6. Management
Supportive care only: The mainstay of treatment is rest, hydration, and symptomatic relief.
Analgesics and antipyretics: Paracetamol or NSAIDs to control pain and fever.
Avoid strenuous activity until symptoms resolve; this helps reduce risk of complications such as myocarditis.
Monitoring: If the patient develops signs of cardiac involvement (palpitations, chest tightness, ECG changes), further evaluation is needed.
7. Prognosis
Excellent prognosis in the vast majority of cases; the condition resolves fully without residual damage.
Recurrences are uncommon but possible.
Serious complications such as myocarditis or pericarditis are rare but require prompt medical attention.
8. Summary Table: Bornholm Disease Overview
9. Conclusion
Bornholm disease is a distinctive and dramatic manifestation of a viral myositis affecting the chest wall and pleura. Its hallmark “gripping” pain may evoke concern for heart or lung disease—but with the right clinical context (viral prodrome, muscle tenderness, epidemic pattern) the diagnosis is often clear. Recognizing it helps avoid unnecessary investigations and reassures patients of a benign outcome
Comment